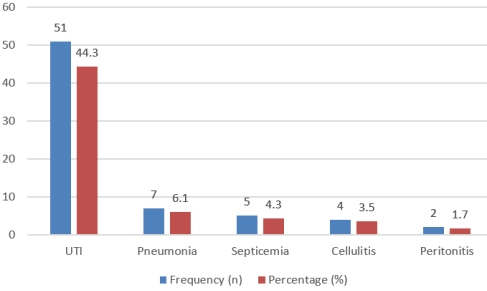
Background: Nephrotic syndrome is a common pediatric renal disorder frequently complicated by infections, which significantly increase morbidity and may influence disease progression. Identifying disease characteristics and determinants of infection is essential for improving management strategies. Methods: This cross-sectional study was conducted in the Department of Pediatric Nephrology at Dhaka Shishu (Children) Hospital from January 2010 to November 2010. A total of 115 children aged 1–13 years diagnosed with nephrotic syndrome were enrolled. Detailed clinical evaluation and laboratory investigations were performed. Data were analyzed to determine the pattern of infections and associated risk factors and a p-value <0.05 was considered statistically significant. Results: The majority of children were between 2–6 years of age, with a mean age of 5.29±2.7 years. Most patients were from rural areas (73.91%) and had poor socioeconomic backgrounds (52.17%). Relapse was observed in 50.44% of cases, while 17.39% were steroid dependent and 15.64% were steroid resistant. Almost all children presented with generalized swelling, proteinuria and oliguria; 26.10% had fever. Urinary tract infection was the most common infection (44.35%), followed by pneumonia (6.09%) and septicemia (4.35%). Steroid dependence (p=0.03), steroid resistance (p=0.001), generalized swelling (p=0.02), low serum albumin (p=0.02) and lower protein–creatinine ratio (p=0.01) were significantly associated with infection. Conclusion: Infection remains a major complication of childhood nephrotic syndrome, particularly among steroid-dependent and steroid-resistant cases. Early identification of high-risk patients is crucial to reduce infectious morbidity and improve outcomes.
| Published in | American Journal of Pediatrics (Volume 12, Issue 1) |
| DOI | 10.11648/j.ajp.20261201.17 |
| Page(s) | 48-54 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Nephrotic Syndrome, Infection, Steroid Dependence, Steroid Resistance, Urinary Tract Infection, Children
Age in years | No. of patients | Percentage |
|---|---|---|
<2 yrs | 4 | 3.48 |
2-6 yrs | 61 | 53.04 |
>6 yrs | 50 | 43.48 |
Socio demographic data | No. of patients | Percentage | |
|---|---|---|---|
Residence | Urban | 30 | 26.09 |
Rural | 85 | 73.91 | |
Socioeconomic status | Poor | 60 | 52.17 |
Average | 49 | 42.61 | |
Well to do | 6 | 5.22 | |
Immunization status | Immunized | 81 | 70.43 |
Not immunized | 34 | 29.57 | |
Mother's education | No education | 53 | 46.09 |
Primary | 40 | 34.78 | |
>Primary | 22 | 19.3 | |
Types of Nephrotic Syndrome | No. of patients | Percentage | |
|---|---|---|---|
1st attack | 19 | 16.52 | |
Relapse | Infrequent relapse | 33 | 28.70 |
Frequent relapse | 25 | 21.74 | |
Steroid dependent | 20 | 17.39 | |
Steroid resistant | 18 | 15.65 | |
Presenting features | No. of Patients | Percentage |
|---|---|---|
Generalized Swelling | 94 | 81.74% |
Proteinuria | 115 | 100% |
Oliguria | 110 | 95.70% |
Hematuria | 9 | 7.80% |
Fever | 30 | 26.10% |
Abdominal pain | 7 | 6.10% |
Sore Throat | 2 | 1.70% |
Risk factors | Infection | χ2 | P value | ||
|---|---|---|---|---|---|
Present | Absent | ||||
Age | <6 years | 28 | 37 | 1.351 | 0.16 |
>6 years | 27 | 23 | |||
Sex | Male | 35 | 46 | 2.340 | 0.09 |
Female | 20 | 14 | |||
Relapse | Present | 46 | 50 | 0.002 | 0.58 |
Absent | 9 | 10 | |||
Steroid dependent | Present | 14 | 06 | 4.771 | 0.03 |
Absent | 41 | 54 | |||
Steroid Resistant | Present | 15 | 3 | 10.782 | 0.001 |
Absent | 40 | 57 | |||
Swelling of the face | Present | 54 | 58 | 0.259 | 0.53 |
Absent | 1 | 2 | |||
Swelling of the legs | Present | 54 | 58 | 0.259 | 0.53 |
Absent | 1 | 20 | |||
Swelling of the genitalia | Absent | 53 | 60 | 2.220 | 0.23 |
Present | 2 | 0 | |||
Generalized swelling | Yes | 15 | 6 | 5.736 | 0.02 |
No | 40 | 54 | |||
Urine Output | Decreased | 54 | 56 | 1.622 | 0.21 |
Not Decreased | 1 | 4 | |||
Fever | Absent | 41 | 44 | 0.022 | 0.53 |
Present | 14 | 16 | |||
Pain abdomen | Absent | 51 | 57 | 0.259 | 0.45 |
Present | 4 | 3 | |||
Vomiting | Absent | 52 | 54 | 0.822 | 0.29 |
Present | 3 | 6 | |||
Skin infection | Absent | 52 | 59 | 1.226 | 0.28 |
Present | 3 | 1 | |||
Sore throat | Absent | 53 | 60 | 20220 | 0.23 |
Present | 2 | 0 | |||
Immunization | Immunized | 41 | 40 | 0.855 | 0.23 |
Not immunized | 14 | 20 | |||
Albumin | <4+ | 1 | 8 | 5.275 | 0.02 |
>4+ | 54 | 52 | |||
RBC | <10 | 41 | 52 | 2.725 | 0.08 |
>10 | 14 | 08 | |||
Protein creatinine ratio | <5 | 16 | 6 | 6.760 | 0.01 |
>5 | 39 | 54 | |||
NS | Nephrotic Syndrome |
UTI | Urinary Tract Infection |
IHC | Immunohistochemistry |
CBC | Complete Blood Count |
ESR | Erythrocyte Sedimentation Rate |
KUB | Kidney–Ureter–Bladder |
SPSS | Statistical Package for the Social Sciences |
HBsAg | Hepatitis B Surface Antigen |
HCV | Hepatitis C Virus |
ELISA | Enzyme-Linked Immunosorbent Assay |
X2 | Chi-square |
| [1] | Eddy AA, Symons JM. Nephrotic syndrome in childhood. The lancet. 2003 Aug 23; 362(9384): 629-39. |
| [2] | Bagga A, Mantan M. Nephrotic syndrome in children. Indian Journal of medical research. 2005 Jul 1; 122(1): 13. |
| [3] | Yap HK, Han EJ, Heng CK, Gong WK. Risk factors for steroid dependency in children with idiopathic nephrotic syndrome. Pediatric Nephrology. 2001 Dec; 16(12): 1049-52. |
| [4] | Soeiro EM, Koch VH, Fujimura MD, Okay Y. Influence of nephrotic state on the infectious profile in childhood idiopathic nephrotic syndrome. Revista do Hospital das Clínicas. 2004 Oct 29; 59(5): 273-8. |
| [5] | Toyabe SI, Cao P, Abe T, Uchiyama M, Akazawa K. Impact of sociocultural factors on hospital length of stay in children with nephrotic syndrome in Japan. Health policy. 2006 May 1; 76(3): 259-65. |
| [6] | Hingorani SR, Weiss NS, Watkins SL. Predictors of peritonitis in children with nephrotic syndrome. Pediatric nephrology. 2002 Aug; 17(8): 678-82. |
| [7] | Alwadhi RK, Mathew JL, Rath B. Clinical profile of children with nephrotic syndrome not on glucorticoid therapy, but presenting with infection. Journal of paediatrics and child health. 2004 Jan; 40(1‐2): 28-32. |
| [8] | Lama G, Luongo I, Tirino G, Borriello A, Carangio C, Salsano ME. T-lymphocyte populations and cytokines in childhood nephrotic syndrome. American Journal of Kidney Diseases. 2002 May 1; 39(5): 958-65. |
| [9] | Olowu WA, Adelusola KA, Adefehinti O. Reversed clinical and morphologic characteristics of idiopathic childhood nephrotic syndrome. 2010. |
| [10] | FE AS, NJ A. Self–care practices of School age children with nephrotic syndrome. Journal of High Institute of Public Health. 2009 Oct 1; 39(4): 709-28. |
| [11] | Uncu N, Bülbül M, Yıldız N, Noyan A, Koşan C, Kavukçu S, Çalışkan S, Gündüz Z, Beşbaş N, Gür Güven A. Primary peritonitis in children with nephrotic syndrome: results of a 5-year multicenter study. European journal of pediatrics. 2010 Jan; 169(1): 73-6. |
| [12] | Niaudet PA. Steroid-sensitive idiopathic nephrotic syndrome in children. Pediatric nephrology. 2004; 5: 543-56. |
| [13] | Webb NJ. Epidemiology and general management of childhood idiopathic nephrotic syndrome. Evidence‐Based Nephrology. 2008 Dec 5: 763-73. |
| [14] | Chang JW, Tsai HL, Wang HH, Yang LY. Clinicopathological features and prognosis of Chinese children with idiopathic nephrotic syndrome between different age groups. European journal of pediatrics. 2009 Oct; 168(10): 1189-94. |
| [15] | Anochie I, Eke F, Okpere A. Childhood nephrotic syndrome: change in pattern and response to steroids. Journal of the National Medical Association. 2006 Dec; 98(12): 1977. |
| [16] | Davutoglu M, Ece A, Bilici M, Dagli A. Steroid responsiveness of children with idiopathic nephrotic syndrome in southeastern region of Turkey. Renal failure. 2007 Jan 1; 29(7): 855-9. |
| [17] | Andersen RF, Thrane N, Noergaard K, Rytter L, Jespersen B, Rittig S. Early age at debut is a predictor of steroid-dependent and frequent relapsing nephrotic syndrome. Pediatric nephrology. 2010 Jul; 25(7): 1299-304. |
| [18] | Roth KS, Amaker BH, Chan JC. Nephrotic syndrome: pathogenesis and management. Pediatrics in review. 2002 Jul 1; 23(7): 237-48. |
| [19] | Kodner C. Nephrotic syndrome in adults: diagnosis and management. American family physician. 2009 Nov 15; 80(10): 1129-34. |
| [20] | Doe JY, Funk M, Mengel M, Doehring E, Ehrich JH. Nephrotic syndrome in African children: lack of evidence for ‘tropical nephrotic syndrome? Nephrology Dialysis Transplantation. 2006 Mar 1; 21(3): 672-6. |
| [21] | Han JW, Lee KY, Hwang JY, Koh DK, Lee JS. Antibody status in children with steroid-sensitive nephrotic syndrome. Yonsei Medical Journal. 2010 Mar 1; 51(2): 239-43. |
| [22] | Bagga A, Hari P, Moudgil A, Jordan SC. Mycophenolate mofetil and prednisolone therapy in children with steroid-dependent nephrotic syndrome. American journal of kidney diseases. 2003 Dec 1; 42(6): 1114-20. |
| [23] | Gipson DS, Massengill SF, Yao L, Nagaraj S, Smoyer WE, Mahan JD, Wigfall D, Miles P, Powell L, Lin JJ, Trachtman H. Management of childhood onset nephrotic syndrome. Pediatrics. 2009 Aug 1; 124(2): 747-57. |
| [24] | Hodson EM. The management of idiopathic nephrotic syndrome in children. Pediatric Drugs. 2003 May; 5(5): 335-49. |
APA Style
Mahmud, S., Ashique, S. S., Kamal, N., Alam, S., Mahjabin, R., et al. (2026). Disease Characteristics and Determinants of Infection Among Children with Nephrotic Syndrome. American Journal of Pediatrics, 12(1), 48-54. https://doi.org/10.11648/j.ajp.20261201.17
ACS Style
Mahmud, S.; Ashique, S. S.; Kamal, N.; Alam, S.; Mahjabin, R., et al. Disease Characteristics and Determinants of Infection Among Children with Nephrotic Syndrome. Am. J. Pediatr. 2026, 12(1), 48-54. doi: 10.11648/j.ajp.20261201.17
@article{10.11648/j.ajp.20261201.17,
author = {Sarwar Mahmud and Shamsi Sumaiya Ashique and Nusrat Kamal and Saidul Alam and Rubana Mahjabin and Moshiur Rahman},
title = {Disease Characteristics and Determinants of Infection Among Children with Nephrotic Syndrome},
journal = {American Journal of Pediatrics},
volume = {12},
number = {1},
pages = {48-54},
doi = {10.11648/j.ajp.20261201.17},
url = {https://doi.org/10.11648/j.ajp.20261201.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20261201.17},
abstract = {Background: Nephrotic syndrome is a common pediatric renal disorder frequently complicated by infections, which significantly increase morbidity and may influence disease progression. Identifying disease characteristics and determinants of infection is essential for improving management strategies. Methods: This cross-sectional study was conducted in the Department of Pediatric Nephrology at Dhaka Shishu (Children) Hospital from January 2010 to November 2010. A total of 115 children aged 1–13 years diagnosed with nephrotic syndrome were enrolled. Detailed clinical evaluation and laboratory investigations were performed. Data were analyzed to determine the pattern of infections and associated risk factors and a p-value <0.05 was considered statistically significant. Results: The majority of children were between 2–6 years of age, with a mean age of 5.29±2.7 years. Most patients were from rural areas (73.91%) and had poor socioeconomic backgrounds (52.17%). Relapse was observed in 50.44% of cases, while 17.39% were steroid dependent and 15.64% were steroid resistant. Almost all children presented with generalized swelling, proteinuria and oliguria; 26.10% had fever. Urinary tract infection was the most common infection (44.35%), followed by pneumonia (6.09%) and septicemia (4.35%). Steroid dependence (p=0.03), steroid resistance (p=0.001), generalized swelling (p=0.02), low serum albumin (p=0.02) and lower protein–creatinine ratio (p=0.01) were significantly associated with infection. Conclusion: Infection remains a major complication of childhood nephrotic syndrome, particularly among steroid-dependent and steroid-resistant cases. Early identification of high-risk patients is crucial to reduce infectious morbidity and improve outcomes.},
year = {2026}
}
TY - JOUR T1 - Disease Characteristics and Determinants of Infection Among Children with Nephrotic Syndrome AU - Sarwar Mahmud AU - Shamsi Sumaiya Ashique AU - Nusrat Kamal AU - Saidul Alam AU - Rubana Mahjabin AU - Moshiur Rahman Y1 - 2026/03/27 PY - 2026 N1 - https://doi.org/10.11648/j.ajp.20261201.17 DO - 10.11648/j.ajp.20261201.17 T2 - American Journal of Pediatrics JF - American Journal of Pediatrics JO - American Journal of Pediatrics SP - 48 EP - 54 PB - Science Publishing Group SN - 2472-0909 UR - https://doi.org/10.11648/j.ajp.20261201.17 AB - Background: Nephrotic syndrome is a common pediatric renal disorder frequently complicated by infections, which significantly increase morbidity and may influence disease progression. Identifying disease characteristics and determinants of infection is essential for improving management strategies. Methods: This cross-sectional study was conducted in the Department of Pediatric Nephrology at Dhaka Shishu (Children) Hospital from January 2010 to November 2010. A total of 115 children aged 1–13 years diagnosed with nephrotic syndrome were enrolled. Detailed clinical evaluation and laboratory investigations were performed. Data were analyzed to determine the pattern of infections and associated risk factors and a p-value <0.05 was considered statistically significant. Results: The majority of children were between 2–6 years of age, with a mean age of 5.29±2.7 years. Most patients were from rural areas (73.91%) and had poor socioeconomic backgrounds (52.17%). Relapse was observed in 50.44% of cases, while 17.39% were steroid dependent and 15.64% were steroid resistant. Almost all children presented with generalized swelling, proteinuria and oliguria; 26.10% had fever. Urinary tract infection was the most common infection (44.35%), followed by pneumonia (6.09%) and septicemia (4.35%). Steroid dependence (p=0.03), steroid resistance (p=0.001), generalized swelling (p=0.02), low serum albumin (p=0.02) and lower protein–creatinine ratio (p=0.01) were significantly associated with infection. Conclusion: Infection remains a major complication of childhood nephrotic syndrome, particularly among steroid-dependent and steroid-resistant cases. Early identification of high-risk patients is crucial to reduce infectious morbidity and improve outcomes. VL - 12 IS - 1 ER -
Department of Paediatrics, National Center for Control of Rheumatic Fever and Heart Diseases, Dhaka, Bangladesh
Department of Paediatrics, National Center for Control of Rheumatic Fever and Heart Diseases, Dhaka, Bangladesh
Department of Paediatrics, National Center for Control of Rheumatic Fever and Heart Diseases, Dhaka, Bangladesh
Department of Cardiology, National Center for Control of Rheumatic Fever and Heart Diseases, Dhaka, Bangladesh
Department of Pediatrics, Dhaka Central International Medical College, Dhaka, Bangladesh
Department of Epidemiology, National Center for Control of Rheumatic Fever & Heart Disease, Dhaka, Bangladesh